A 60F with Megaloblastic Anemia
Note - This is an online e log book to discuss our patient's de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centred online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment.
DOA - 27/11/2023
CHIEF COMPLAINTS:
Fever since 1 week
Palpitations since 1 week
Generalised weakness since 4 days
Blood in stools since 3 days
Chest pain and tightness since 4 days
HISTORY OF PRESENTING ILLNESS
The patient was apparently asymptomatic 1 week ago and then she developed fever which is sudden in onset, high grade, associated with chills and rigors, relieved temporarily on medication.
Palpitations are present since 1 week which are regular and associated with chest discomfort
There is h/o shortness of breath on exertion which is progressive (grade 2 to grade 3). No orthopnea, or PND.
There is associated generalised weakness since 4 days and blood in stools since 3 days.
There is no h/o vomitings, loose stools, pain abdomen, giddiness.
PAST HISTORY
N/k/c/o DM, HTN, Asthma, TB, Epilepsy, CAD, CVA
There is h/o tubectomy
PERSONAL HISTORY
Diet mixed
Appetite normal
Sleep adequate
Bowel movement- Constipation present, Bladder regular
Addictions - None
GENERAL EXAMINATION
Pt is conscious, coherent and cooperative and well oriented to time, place and person.
No cyanosis, clubbing, lymphadenopathy and edema
Pallor present
Icterus present

.





Vitals on admission -
Temp - 98F
BP - 130/70 mm hg
PR - 98bpm
RR- 22cpm
Grbs - 131mg/dl
SpO2 - 90% @ RA
SYSTEMIC EXAMINATION
CVS - S1 loud, S2 heard, JVP raised, systolic murmur present
RS - trachea - central , bilateral air entry +, NVBS heard, no added sounds
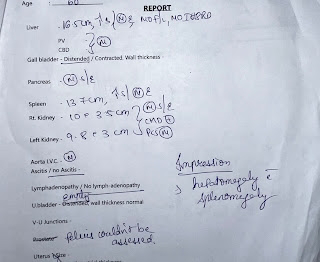
PER ABDOMEN - soft, non tender, hepatomegaly present, bowel sounds heard
CNS - NFND

INVESTIGATIONS



PROVISIONAL DIAGNOSIS
Megaloblastic Anemia
TREATMENT
27/11/23-
1 unit PRBC Transfusion
Inj Pan 40mg IV OD
Inj Iron sucrose 200mg in 100ml NS IV OD
Inj Vitcofol 1500mg in 100ml NS IV OD
Strict I/O charting, monitor vitals, inform sos
28/11/23-
1 unit PRBC transfusion
Inj Ceftriaxone 2g IV BD
Cap Doxycycline 100mg PO BD
Inj Pan 40mg IV OD
Inj Iron sucrose 200mg in 100ml NS IV OD
Inj Vitcofol 1500mg in 100ml NS IV OD
Strict I/O charting, monitor vitals, inform sos
OSCE
What are the causes of tear drop cells/dacrocytes in the peripheral smear?
Seen in -
Iron deficiency, Vitamin B12 deficiency, Myelophthisic anemia , Myelofibrosis. They can also occur as an artefact in blood smear preparation with all pointed ends facing one side

Comments
Post a Comment